VISIT ANY FACEBOOK IVF GROUP (DON'T. PLEASE DON'T) and you'll see countless posts about embryo grading. Usually, people are after anecdotes and reassurance that a “poorly” graded embryo can become a healthy baby.
But, as you'll realise once you've read this, it'd probably be better if FB IVF groups stuck to a remit of “posting photos of babies surrounded by IVF needles” and “writing inspirational messages about how you can DO THIS and you GOT THIS”.
Snarky? Me? OK maybe a little bit… but only because I've seen just what damaging nonsense appears whenever someone asks about embryo grades (or myriad other vaguely sciencey IVF-related topics).
So rather than go down a loooooong rabbit hole that'll benefit Zuckerberg way more than it'll benefit you, read this article instead. It'll give you answers to everything you wanted to know, including:
- What does embryo grading do? How does it work?
- What's the difference between Day 3 and Day 5 embryo grading?
- How do I interpret the results?
- What's the “perfect” embryo grade?
- What's a “bad” embryo grade?
- Does a “bad” embryo grade mean it definitely won't implant/survive?
Aaaaaand START!
What's the difference between a Day 3 and a Day 5 embryo?
Read this article on Day 3 vs Day 5 embryos.
What’s the purpose of embryo grading?
Embryo grading is a largely subjective assessment of the “morphology” (the visual appearance) of embryos under a microscope. When embryologists grade each embryo, they’re looking out for certain visual characteristics that imply it has a better chance of implantation, pregnancy, and birth.
What does it mean when an embryo has a good grade?
If you’re smugly downloading Oxbridge scholarship forms while playing classical music to the morphologically perfect embryo in your uterus, you can wipe that self-satisfied smile off your face right now! An embryo grade can do one thing and one thing only: assess its potential for becoming a baby one day.
Your baby’s intelligence and gorgeousness have nothing to do with embryo grade. And remember that chromosomal normality is also separate: a stunning embryo could still be chromosomally abnormal. More on this next.
Does embryo grading discover chromosomal abnormalities too?
An embryo that has the best grade possible could still be “aneuploid” – that is, it could have the wrong number of chromosomes. Aneuploid embryos are far more likely to end in miscarriage or a failed treatment cycle – or, if a baby is born, it’s far more likely to have a condition like Down’s Syndrome.
A poorly graded embryo that’s chromosomally normal (“euploid”) has a greater chance of survival than a highly graded embryo that’s chromosomally abnormal (“aneuploid”).
Unfortunately, embryo grading can’t determine whether the embryos have any chromosomal abnormalities. To find out about the state of your embryos’ chromosomes, you need to do something called “pre-implantation genetic screening” (PGS).
Sod’s law dictates that PGS is extremely expensive and has its own set of drawbacks. You can read about the pros and cons of PGS here.
You might be wondering if there's any kind of link between embryo grades and chromosomal abnormalities. After all, PGS Is expensive and has its drawbacks, so it'd be good to know if an embryo's grade can give a clue to its chromosomal make-up.
Unfortunately, the answer is “not really”. Setting aside the fact that embryo grading is largely subjective and two embryologists can easily give different grades to the same embryo, there’s very weak (and therefore not to be taken seriously) evidence for a link between poorly graded Day 5 embryos and chromosome issues.
This study, for example, found that “Morphology and aneuploidy are linked at the blastocyst stage. However, the association is weak, and consequently, morphologic analysis cannot be relied on to ensure transfer of chromosomally normal embryos. A significant proportion of aneuploid embryos are capable of achieving the highest morphologic scores, and some euploid [chromosomally normal] embryos are of poor morphology.”
So basically: if your embryo grades aren’t top notch, it mayyybe increases the risk that those embryos have chromosomal abnormalities. But there are plenty of examples to the contrary.
This study reported the same findings: “… this analysis was able to confirm the moderate association between aneuploidy and several distinct features of blastocyst morphology…
“However, this association was weak with a significant proportion of aneuploid embryos capable of achieving the hidghest morphologic scores (52% of excellent and good quality blastocysts).”
The study concluded that embryo grading can’t be used as a proxy for PGS when it comes to assessing whether an embryo has chromosomal abnormalities or not.
Now that you know how embryo grading works, what its drawbacks are, and what it can tell you, it’s time to look into the specifics of Day 3 embryo grading and Day 5 embryo grading.
Day 3 embryo grading
How does Day 3 embryo grading work?
First, bear in mind the caveats of embryo grading:
- It’s largely subjective because it’s based on what the embryologist sees.
- It’s perfectly possible that an embryo with a “poor” grade results in a pregnancy (and birth), and it’s just as possible that one with a “perfect” grade does not.
- Embryo grading can’t tell you what’s going on inside the embryo genetically. (You need PGS for that, although – as noted above – PGS comes with its own set of criticisms.)
That out the way, let’s discuss embryo grading!
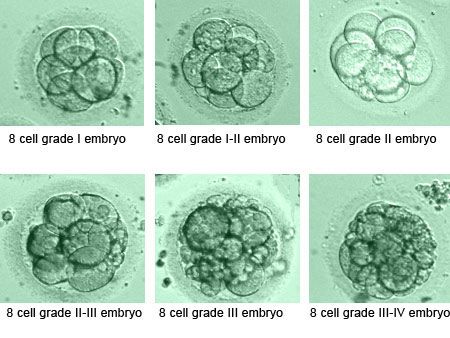
When Day 3 embryos are ready to be transferred (or ready to be frozen), they’re viewed under a microscope and graded accorded to three criteria:
- The number of cells in the embryo (objective). A Day 3 embryo that’s growing normally should contain between 6 and 10 cells. (These embryos are more likely to grow, develop and survive compared to embryos with fewer cells at this stage.)
- How much “fragmentation” can be seen in the cells (subjective assessment). As mentioned earlier, bits of cell can break off as they divide (“cleave”) – and more fragmentation is associated with a lower-quality embryo.
Generally, clinics believe that <10% fragmentation is good, 10–25% is OK, and >25% is poor.
Fragmentation is often scored from 1 to 4 – where “4” (the best score) implies little or no fragmentation and “1” implies a high percentage of fragmentation… although some clinics switch the scoring to be the other way around. - Whether the cells are “symmetrical” – i.e. that they’re all roughly the same size as each other (subjective assessment). When cells lack symmetry, it’s associated with a lower-quality embryo.
When the cells have complete symmetry, clinics are very happy! Anything >50% symmetry is generally considered OK, and <50% is poor.
Symmetry is also often scored from 1 to 4 – where “4” implies near-perfect symmetry and “1” implies poor symmetry… although some clinics switch the scoring to be the other way around.
Deciphering your Day 3 embryo grades
Different clinics have different ways of reporting embryo grading. A common method is to provide a grade like this for each embryo:
8c 3/2
This means “8 cells”, “grade 3 fragmentation” and “grade 2 symmetry”.
(Or for some clinics it might mean “8 cells”, “grade 3 symmetry” and “grade 2 fragmentation”.)
Some clinics will combine/average out the grades for fragmentation and symmetry, providing just one number. And remember: the numbers might be the other way around for your particular clinic. That is, “1” could be good instead of bad.
Oh and by the way, some clinics just prefer to tell you “good”, “OK” and “a bit iffy” instead. Ask your clinic how they choose to do things.
What’s the “perfect” Day 3 embryo grade?
Assuming “4” is best and “1” is worst, the perfect embryo grade would be:
6c 4/4
Or
8c 4/4
Or
10c 4/4
What’s the lowest “grade” an embryologist would consider transferring (for Day 3 embryos)?
It seems most embryologists agree that anything less than a six-cell embryo is considered “poor quality” – as is an embryo that scores “2” or lower on fragmentation and/or symmetry. But clinics have different rules for which they’ll consider freezing/transferring. For example, some might be up for transferring a 4c 3/2 while others wouldn’t; some might be happy to freeze a 6c 2/2 while others wouldn’t.
It also depends on the overall “batch” of embryos from the patient: if you have six high-quality embryos and one relatively poor-quality embryo, that poor-quality embryo is more likely to be discarded than if you have a batch of only poor-quality embryos.
The issue is complicated further by the fact that not all embryologists believe that all three factors (cell number, fragmentation and symmetry) are useful predictors of success. See the next question for more on this.
Are doctors right to be generally dismissive of “poorer quality” embryos? I haven’t done too much reading around this, but from what I can tell…
- Poor-quality Day 3 embryos are unlikely to do a 180 and become high-quality blastocysts.
- But if they do become “good enough” blastocysts, they have a good chance for implantation and successful pregnancy.
(See this cohort study, for example.)
That suggests there’s a good argument for Day 5 embryo transfers rather than Day 3, because it gives a chance for the Day 3-ers to catch up rather than be discarded. It also means PGS can be done for chromosomal abnormalities (as embryologists tend to prefer doing PGS on Day 5 embryos). But THEN you have the issue that a relatively poor-quality Day 3 might survive if transferred immediately but will perish if left to grow further in the petri dish.
Ultimately, the answer to “What’s the lowest ‘grade’ an embryologist would consider transferring (for Day 3 embryos)?” should be individualised, and it should depend on how many eggs, embryos and funds you have.
One more thing to mention: success rates. Poorly graded embryos, as we know, have a lower success rate when it comes to implantation and live births, We also know that poorly graded embryos still have a chance of successful implantation/birth. But if a clinic decides to start transferring more “1s” or “2s” (perhaps for couples with poor-quality batches where those 1s and 2s are their only hope), their success rate is going to decrease compared to other clinics.
Being an embryologist sure ain’t easy.
What’s more important: number of cells, fragmentation, or symmetry?
Arrrghh I think we’re in one of those “lots of studies show lots of different things” scenarios.
From all my reading, it seems cell number and fragmentation are both more important than symmetry. What’s more, cell number and fragmentation levels may be linked to each other – that is, a Day 3 embryo with a suboptimal number of cells is also more likely to have a higher degree of fragmentation.
(Here are a few of the studies and articles I read: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4831697/ and https://www.fertstert.org/article/S0015-0282(03)01308-6/fulltext and https://www.arcfertility.com/understanding-embryo-grading/.)
But I’ve yet to get to the bottom of this one, and I’ll update the page if/when I ever do so!
It’s a bloomin’ minefield.
Let’s move on to a topic that’s just as contentious: Day 5 embryos.

Day 5 embryo grading
How are Day 5 (or Day 6) “blastocyst stage” embryos graded?
Before we get started, it’s caveat time again! As with Day 3 embryos…
- It’s largely subjective because it’s based on what the embryologist sees.
- It’s perfectly possible that an embryo with a “poor” grade results in a pregnancy (and birth), and it’s just as possible that one with a “perfect” grade does not.
- Embryo grading can’t tell you what’s going on inside the embryo genetically. (You need PGS for that, although – as noted above – PGS comes with its own set of criticisms.)
Back to embryo grading!
When Day 5 or 6 embryos are ready for transfer (or ready to be frozen), they’re viewed under a microscope and graded.
Many clinics use the “Gardner blastocyst grading system” (or a variation of it), which involves assigning three separate scores to each embryo:
Score 1: the level of expansion of the embryo (scored 1–6) at Day 5 or Day 6. An embryo that can’t fully expand and grow in the petri dish won’t be able to develop into a baby.
Here are what the different “expansion grades” mean (you might need to remind yourself of “The stages of embryo development” process at the start):
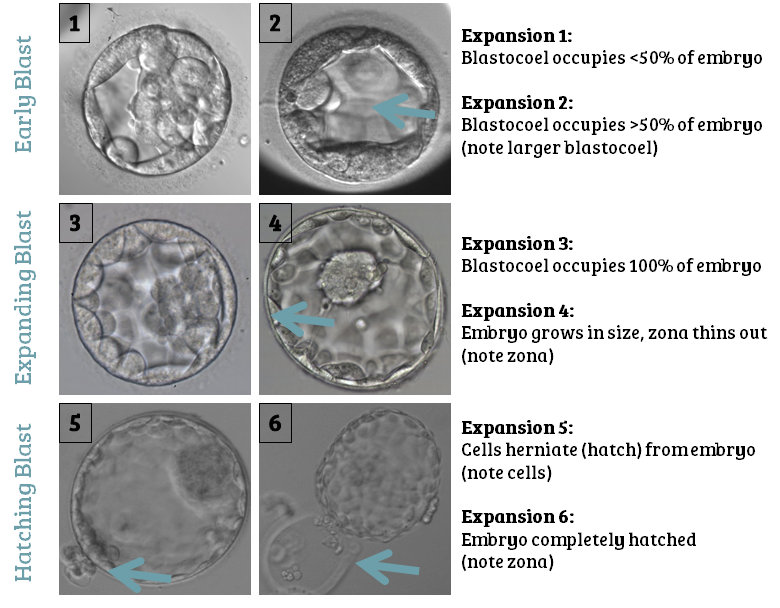
Note: the “zona” mentioned above refers to “zona pellucida” – the blastocyst’s protective outer membrane, which thins as the blastocyst expands. The blastocyst eventually breaks free from this membrane (“hatches”), to enable it to implant properly once it’s in the uterus.
Also note: “Stage/Expansion 6” isn’t necessarily the best. Many clinics believe that the best blastocysts are the “Stage 5s” that haven’t completely hatched yet.
Score 2: the quality of the inner cell mass (scored A–C). The inner cell mass (ICM) is the part of the embryo that develops into a foetus. ICM quality relates to the number of cells and how compacted they are: you want a lot of cells, and you want them to be tightly packed.
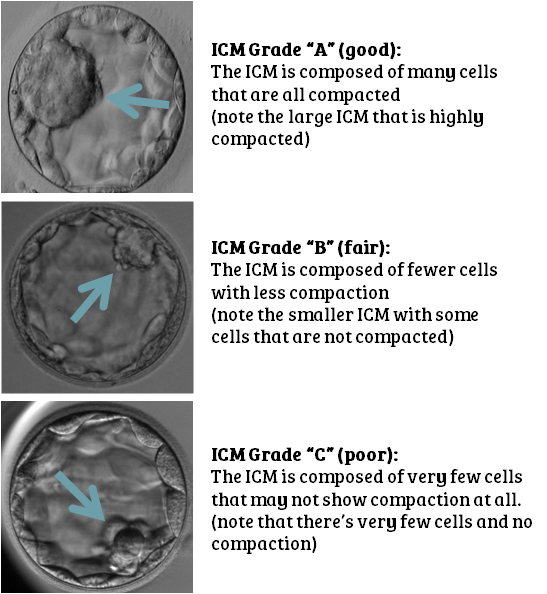
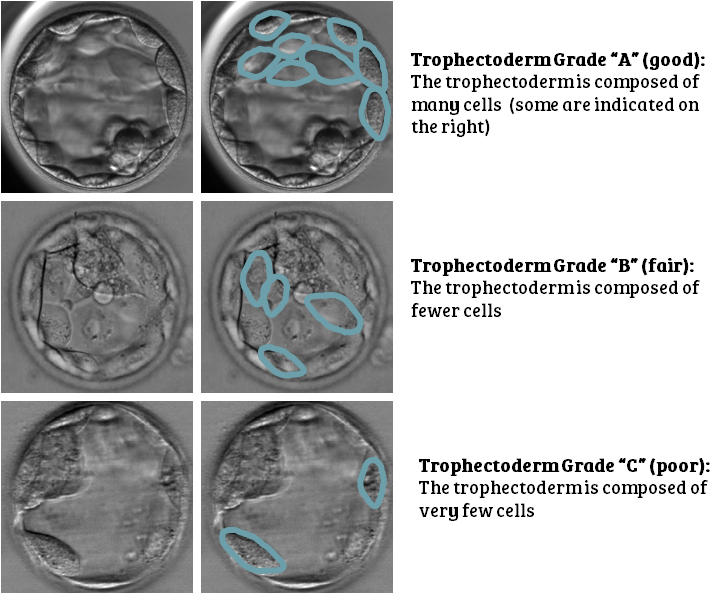
Score 3: the quality of the trophectoderm (scored A–C). The trophectoderm is the part of the embryo that develops into the placenta. As with the ICM, you ideally want a lot of cells that are tightly compacted.
Note: some clinics will also have Grade D, for a very poor-quality ICM/trophectoderm. And some clinics will give the ICM/trophectoderm grades “+” or “-” ratings too (e.g. “B+”). And some clinics will convert their letter gradings into numbers – just to be different.
What’s the “perfect” Day 5 embryo grade?
Most clinics would agree that “5AA” (or “5A+A+” for some clinics) is a pretty impressive embryo. Clinics are also more likely to value Day 5 embryos over Day 6 embryos, so if you have a 5AA for Day 6 and a 5AB for Day 5, they may well select the 5AB from Day 5.
(Having said that, recent research has shown that there’s very little difference in outcomes between transferring a Day 5 embryo and a Day 6 embryo. If you’re interested in learning more about this, here’s a massive, fascinating post. (Read the section called: “Timing of blast development: Day 5, 6 or 7?”)
Here’s what a hatching 5AA blastocyst looks like:
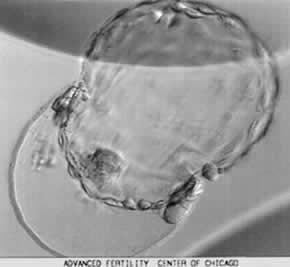
But please remember the following:
- Even a 5AA embryo can result in no pregnancy. There are no certainties.
- And, of course, something like a 3AB embryo can lead to a baby.
- Any embryo can still have chromosomal abnormalities (which can only get picked up with PGS rather than embryo grading).
What’s most important when it comes to the blastocyst grade: embryo expansion, inner cell mass, or trophectoderm?
Let’s say you’ve ended up with the following embryos:
5BB, 2AA, 4AB, 4BA
Assuming there are no chromosomal abnormalities with any of them, which embryo would an embryologist choose to transfer first?
As you’d imagine, there’s no clear consensus.
This fantastic report compared multiple studies into embryo grading, and learnt the following:
- One study found that embryo expansion was the most important factor
- Two studies found that the ICM grade was the most important factor
- Four studies found that the trophectoderm grade was the most important factor
- One study found that NONE of the blastocyst features related to implantation potential!
Embryologists do stress that they use the grading system as a tool to help determine which blastocyst(s) to transfer or freeze, but they don’t rely solely on the grading system. They’ll also consider your age, fertility history and other information to determine which embryo(s) to transfer or freeze.
It’s also important to remember that if an embryo has a good grade in one category, it’s more likely to have good grades in the other two. That is, an embryo that’s at Stage 4 of expansion on Day 5 is more likely to have A or B grades for both the ICM and trophectoderm in a healthy embryo. You’re less likely to see something like “4CC” or “1AA”. Although, of course, there are always plenty of exceptions.
What’s the lowest “grade” an embryologist would consider transferring (for Day 5 or Day 6 embryos)?
As with Day 3 embryos, it depends on the clinic. And always bear in mind that embryo grading is subjective, so a “C” grade for ICM at one clinic might be a “B” at another. Something else to be aware of is that not all clinics use the same grading system (or, at the very least, many of them modify the Gardner system), so – again – it’s difficult to make any clinic-wide claims here.
All I really can say is that most clinics look for blastocyst expansion of at least “3”, and trophectoderm/ICM grades of at least C (but usually A or B). Some clinics will attempt to transfer fresh embryos if they’re Stage 1 or 2 / Grade C, but they’re less likely to freeze them (as it’s believed they wouldn’t survive the freeze-thaw process).
Here’s what a 2BC embryo looks like:

Are they right to be dismissive of “poorer quality” embryos? No, according to a report called “Is a ‘C’ a failing grade?” Not only does this report highlight just how subjective/biased embryo grading is, but it also shows how Stage 1 or 2 / Grade C embryos can and do result in live births. The live birth rate is lower – as you’d expect – but it’s not insignificant.
We also shouldn’t forget (as if I’d let you!) that embryo grading is only part of the equation. If it has abnormal chromosomes, the world’s most beautiful embryo is far less likely to make it.
So… as with Day 3 embryos, the answer to “What’s the lowest ‘grade’ an embryologist would consider transferring (for Day 5 or Day 6 embryos)?” should be individualised, and it should depend on how many eggs, embryos and funds you have. If you have tons of good-quality embryos and a few not-so-great ones, transfer a good one. If you have a few poor-quality embryos, you and your clinic will need to decide if it’s worth doing PGS (especially considering the cost to you), or if it’s worth transferring them or starting from scratch with a new cycle.
And again, there’s the issue of success rates. Whether you’re on the NHS or going down the private route, poorly graded embryos are less likely to implant and lead to a live birth, so if a clinic makes the decision to transfer more “Cs”, their success rate is going to decrease.
If a clinic is planning to transfer (or freeze) a Day 5 blastocyst, will the embryo also be graded on Day 3?
For clinics that prefer Day 5 transfers, they’ll often leave young embryos alone to do their growing thing (as long as there’s no reason to believe those embryos will be struggling). But it really depends on the clinic.
We’re done!
If you have any questions about this article, email me and let me know!
