IF YOUR MANTRA IN LIFE IS LESS “GO WITH THE FLOW” AND MORE “TELL ME EVERY FREAKING THING THAT'S GOING TO HAPPEN TO ME, GODDAMIT”, then this is the article for you. It presents the ENTIRE IVF process – from paperwork and weigh-ins right the way through to a (fingers crossed) positive pregnancy test.
To be honest, I think everyone considering or embarking on IVF should read this – regardless of how detail-oriented you are. It will help prepare you for what’s to come, reassure you about certain weird aspects of the process, answer questions you might have, and explain why the doctor is prescribing certain meds or telling you to go for your fifth blood test of the week.
Feel free to skip the sciencey explanations if you like – although that does mean you’ll be missing out on some of my best jokes.
Before you get started on the article below, it's helpful to know what goes on in a “normal” menstrual cycle: you'll then find it easier to understand the whats and whys of the IVF process below. Read this article for a full explanation of a “normal” menstrual cycle.
Click here to download a quick printable summary of the entire process – plus a jam-packed IVF glossary. (Opens in a new window.)

Pre-IVF #1: paperwork, weigh-ins, etc.
Everyone’s route to IVF is slightly different, but it normally involves a referral from your GP and a big ol’ collection of appointments with the fertility department that you were referred to. (If you've decided to be treated privately, you won't need a referral: you can just contact the clinic directly.) There’ll be paperwork, weigh-ins, and possibly a few blood tests and sperm samples to determine if IVF is definitely the right route for you. (Some of the blood tests might then be repeated during Pre-IVF step 3 below.) Your partner will need to be at these appointments with you.
Sometimes, you’ll have an appointment and the doctor will say (after you’ve been waiting 1.5 hours in the waiting room), “I can’t remember why I arranged this appointment with you. Hmmm… no… it’s not coming back to me.” Maybe – hopefully – this just happened to me and it’ll never happen again.
How long does it take to go from “paperwork, weigh-ins, etc.” to the next step?
If you’re with the NHS for your treatment, you may have to wait a few months between this stage and the next one (“Pre-IVF step 2”). If you're being treated privately, there'll be much less time to twiddle your thumbs.
While you’re waiting, you might be instructed to make some lifestyle changes: some people need to quit smoking, while others need to get their BMI down or up to an acceptable level.
Pre-IVF #2: have a period
Once the clinic or hospital is ready to give you fertility treatment, you’ll probably have another appointment where they welcome you, ask you to sign a few more bits and pieces, and tell you that your very first task will be to get your period.
That’s because you’ll need to have some pre-IVF blood tests and a scan on about day 3 of your period, in order to help the doctors understand a bit more about the workings of your body and its likelihood of responding to various treatments. (There’s more on this in Pre-IVF step 3, below.)
Depending on where you’re getting treatment and your particular situation, you’ll either go about your month as normal and call them up as soon as Aunt Flo makes an appearance, or (especially if you have irregular/no periods) you’ll go on the contraceptive pill for a month and give them a ring as soon as Fake Aunt Flo makes herself known. Some clinics like to get you on the pill purely for reasons of “scheduling convenience”.

Pre-IVF #3: “baseline” tests
“Day 3” is the third day of bleeding. What usually happens is this: on the first day that you start bleeding (which means “full flow – not just spotting”), you’ll call up the clinic or hospital and tell them you’ve started your period. They’ll then book you in for your “day 3” tests and scan two days later.
On that day, you’ll go in for some blood tests and a “transvaginal ultrasound scan”. Yep… on your grossest day of the month, you’ll have a doctor probing around in there to check on the state of your ovaries. It'll be nowhere near as awkward or disgusting as you think: promise.
What happens if “day 3” falls on a weekend?
Your clinic might be open for these sorts of tests, or they’ll just book you in for the next available weekday. It doesn’t have to be day 3 necessarily – it just needs to be around the time when your ovaries are quiet and your hormone levels are meant to be in their “resting” state. More on this below.
Why do I have the baseline tests?
Before you begin fertility treatment, your doctors will need to know a bit more about the quantity and quality of your eggs. They need to know this for a few reasons:
- So they can create a customised treatment plan (“protocol”) for you. (If you have a small number of eggs, for example, you may need more aggressive treatment to get enough of them growing.)
- So they can identify if you’re at risk of Ovarian Hyperstimulation Syndrome (OHSS), and tweak the treatment they have planned for you.
- In order to assess your likelihood of conceiving via IVF, and make you aware of your chances of success.
The day 3 tests tell them what they need to know.
If you want to understand more about why egg quality and egg count matter so much (and they really do), read this.
What gets tested?
Depending on the hospital/clinic, you’ll have some or all of the following:
- FSH level blood test
- Oestradiol level blood test
- AMH level blood test
- Antral follicle count scan (the transvaginal ultrasound scan mentioned above)
The links above give you way more information about why these hormones get tested, and what they indicate about your egg quantity/quality.
Why day 3?
On day 3, your uterus should be “resting” and calm, your egg-containing follicles won't have started growing yet, and your hormones will be in “unaggravated mode”. It's the perfect time for the doctors to accurately assess your egg situation by looking at these hormones and seeing what they’re up to.

It’s a similar situation with your ultrasound scan: when everything is resting and peaceful, it’s the best time to look at how many follicles there are and what they’re up to.
What happens if my “day 3” test results are abnormal/bad?
Unless you’re over a certain age (in which case you probably wouldn’t be accepted for IVF treatment anyway), an “abnormal” or “bad” result normally means you’ll be put on a certain “protocol” or tested/monitored more closely in case various issues crop up. (For example, if you have a sky-high AMH level, it means you might be at risk of OHSS – so they’ll keep an eye on you for signs and symptoms.)
Remember: if you’re having fertility treatment for reasons relating to your own fertility (rather than your partner’s), there's a chance at least one of these results won’t be perfect anyway.
Read the individual pages on each test for more information about the test results and what they mean:
Some doctors will repeat a couple of tests if they’re suspicious that the initial results were inaccurate.

Pre-IVF #4 (sometimes): various tests
You may or may not have:
- A HyCoSy (“hysterosalpingo-contrast sonography” for fans of big words), which is a non-invasive ultrasound procedure that checks your uterus and fallopian tubes, and can detect blockages in your tubes. HyCoSy is similar to HSG – and they’re both screening tests, not diagnostic tests.
If any blockages are detected, you then might have a diagnostic test (such as a laparoscopy or hysteroscopy) to find out why. IVF bypasses the fallopian tubes (embryos are transferred directly to your uterus), which means that blocked tubes – while it’s useful to know that you have them – won’t be an issue. - An HSG (hysterosalpingogram), which is very similar to a HyCoSy, but involves x-rays rather than ultrasound.
- A hysteroscopy, which is all about looking at your uterus to check that it’s healthy and ready to carry a baby. If any problems are detected (like fibroids or polyps), they’ll need to be dealt with before you start IVF.
Bear in mind what NICE says about hysteroscopy: “Women should not be offered hysteroscopy on its own as part of the initial investigation unless clinically indicated because the effectiveness of surgical treatment of uterine abnormalities on improving pregnancy rates has not been established.” - A laparoscopy, which is a surgical procedure where the surgeon uses a laparoscope – a small tube that has a light source and a camera – to access the inside of the pelvis or abdomen without needing to make large incisions in the skin. The laparoscope relays images to a monitor and can diagnose a variety of conditions. It can also be used to carry out surgical procedures (such as removing a damaged or diseased organ), or removing a tissue sample for further testing (biopsy). Laparoscopy is carried out under general anaesthetic
- A dummy embryo transfer, which is a trial run of the actual embryo transfer. It allows the doctors to determine the best “route” to the ideal embryo landing place in your uterus, and check for any issues that could make for a tricky transfer (like scar tissue).
Whoop: you're now ready to start IVF treatment!
IVF #1: taking control of your menstrual cycle
- The goal: reset your menstrual cycle
- Approximate time taken: 7–10 days (for long protocol); 0 days (for short protocol)
- Approximate number of appointments needed: 2 (for long protocol); 1 (for short protocol)
- Potential side effects: menopause-like symptoms (for long protocol); nada – for now (for short protocol)
While no one plants a flag on your pituitary gland and triumphantly declares, “This is ALL MINE now, ha ha haaaaaa”, it can sometimes feel that way – especially when the drugs start making you feel all sorts of deranged, hot-tempered emotions that you never knew existed.
“The medical overlords are really screwing with me today,” you’ll occasionally think to yourself – before you start laughing hysterically or sobbing uncontrollably (or both)*. The first proper stage of IVF involves getting your body prepared, and it can get rather technical indeed…
*I’m exaggerating for comic(ish) effect, but you’ll soon see why some women do start to act like they’ve had a booster pack of PMS installed in their brains.
Why do they need to take control of my menstrual cycle?
In normal, run-of-the-mill (i.e. natural) ovulation, just one mature egg is released into the fallopian tube each month. And providing you and your partner don’t have any fertility issues, the process works great if pregnancy is the end goal: every 28 days or so, one mature egg will be released, your app/iCal/pee stick/intuition will tell you that you’re ovulating, and you’ll get jiggy in the bedroom for the next few days.
With this method (i.e. the quaint, old-fashioned way of making a baby), you have a 15–25% chance of getting pregnant each month, depending on your age – and most non-fertility-compromised couples find themselves up the duff within six months.
There are a couple of problems with this method when it comes to IVF:
- The doctors don’t want just one measly egg: they want heaps of ‘em from you. Why? Because lots of eggs mean a better chance that at least one of them can be fertilised and placed back in your uterus. Those eggs need to be ready for fertilisation at around the same time, though, so that they can all be collected together. When the doctors take control of your menstrual cycle, they can make sure all your egg-containing follicles grow at the same time and speed as each other.
- The doctors need to be able to know exactly when your eggs will be ready for retrieval – so that they be ready and waiting with baseball mitts to catch them all as they leap out of your body, ready for some hot-n-heavy petri dish action. You therefore don’t want to start ovulating naturally before IVF begins, because it means that when IVF does begin, you’ll have a nice big mess of timings and confusion. By taking control of your menstrual cycle, doctors are able to determine when to start the process of growing your follicles.
How do they actually take over my menstrual cycle?
There are two main ways: the “long protocol” and the “short protocol”. (There’s also a less-common protocol called “microdose flare protocol”.) Which protocol will you be on? That depends on a number of factors, and soon I'll outline them all in a post about long protocols vs short protocols.
The long protocol (also known as “downregulation”)
Downregulation basically sets your menstrual cycle to zero, and it’s not all that dissimilar from the menopause – albeit a temporary one. Cue occasional menopausal symptoms, such as hot flushes, night sweats, vaginal dryness, acne, sore muscles, forgetfulness, minor depression and headaches. Don’t worry about this too much in advance, though: many women get no side effects whatsoever.
From a science-y perspective, downregulation prevents the release of the hormones FSH and LH from the pituitary gland – which has the effect of preventing spontaneous ovulation. Oestradiol production also grinds to a halt. In practice, this means the following:
- You’ll take drugs as injections or a sniffer spray for 7–10 days – and you’ll start taking these drugs at a specific point in your menstrual cycle (usually on day 1, 2 or 21). The downregulation drugs you’ll take are called “gonadotrophin-releasing hormone (GnRH) agonists”. Brand names include:
Suprecur (generic name: buserelin): nasal spray
Suprefact (generic name: buserelin): injections
Lupron (generic name: leuprolide): injections
Synarel (generic name: nafarelin): nasal spray - After 7–10 days, you’ll have a blood test to check that your oestradiol level is low, and you’ll also have a transvaginal ultrasound examination (a scan) to make sure your ovaries are “quiet” and the lining of your uterus is thin.
- And THEN you can get started on “ovarian stimulation” (i.e. the proper bit of IVF)!
FYI… some clinics and hospitals will ask you to go on the contraceptive pill the preceding month, for purposes of “scheduling convenience”. It means they (and you) can know exactly when your period will arrive – and, therefore, when to book you in to start downregulation. Another reason might also be to prevent the creation of cysts, which can happen with natural cycles.
Sometimes you’ll be prescribed something that’s similar to the contractive pill but isn’t one. Names for these pills include Provera and Norethisterone.
The short protocol
The short protocol is – unsurprisingly – shorter, and it gets you started on “proper” IVF almost immediately. Here’s what happens:
- Usually on day 3 of your period, you’ll have a transvaginal ultrasound examination (a scan) to check that there aren’t any pesky cysts on your ovaries and that your uterus lining is nice and thin. You’ll also have a blood test to check that your oestradiol level is low.
As with the long protocol, some clinics and hospitals will ask you to go on the contraceptive pill the preceding month, for purposes of “scheduling convenience”. Another reason might also be to prevent the creation of cysts, which can happen with natural cycles. Sometimes you’ll be prescribed something that’s similar to the contractive pill but isn’t one. Names for these pills include Provera and Norethisterone. - If the scan and blood test indicate you’re ready, you’ll begin the “ovarian stimulation” phase right away.
What happens if I don’t have a menstrual cycle to take control of?
I didn’t either: my periods stopped when I was 15 and they never returned again. (Something to do with a “sticky hypothalamus”, apparently.) You’ll still go on the long or short protocol, and your clinic will decide whether you should be put on the contraceptive pill first (to bring about a bleed).
Worried you'll never remember all this information? Click here to download a quick printable summary of the entire process – plus a jam-packed IVF glossary. (Opens in a new window.)
IVF #2: ovarian stimulation
- The goal: end up with a decent number of mature eggs, ready to be fertilised
- Approximate time taken: 10–12 days
- Approximate number of appointments needed: 2–7 (ish – depending on what your follicles are up to and what your blood test results show)
- Potential side effects: headache, nausea, vomiting, mild stomach pain, dizziness, bloating, injection site reactions (redness, bruising, etc.), breast swelling/tenderness, runny or stuffy nose, sore throat, acne, skin rash
FINALLY, right?!
As mentioned earlier, a “normal” ovulation cycle usually results in one dominant egg-containing follicle – i.e. one big hunk of a follicle that releases a mature egg into the fallopian tube, ready to be fertilised. In an IVF cycle, the goal is to have as many big hunky follicles as possible – because it’ll increase your odds of success with treatment.
Mathematical formula(ish) time!
- Lots of follicles = lots of eggs (most follicles in your ovaries contain an egg)
- Lots of eggs + sperm = lots of possibilities to have at least one (preferably a few) viable embryo(s)
Most hospitals and clinics aim for around ten big follicles – and to achieve this you’ll start giving yourself injections of either follicle-stimulating hormone (FSH) (also known as follitropins) or a combination of FSH and luteinising hormone (LH) (known collectively as human menopausal gonadotrophins – or hMG).
An uninterfered-with female body produces FSH and LH naturally. With IVF, however, you’ll be given a more prolonged dose of FSH (or FSH and LH) than your body would normally produce, in order to get loads of follicles to grow rather than just one.
Both FSH and hMG injections will bypass the hypothalamus and pituitary glands to directly stimulate your follicles in the ovaries.
Which stimulation medication will I be on?
Common FSH-only medications include:
- Follistim
- Gonal-F
- Bravelle
- Bemfola
- Pergoveris
- Puregon
Common FSH+LH medications (known as human menopausal gonadotrophin or hMG) include:
- Repronex
- Menopur
There are slight variations in how you take each type of medication, but the general gist is: you’ll be stabbing yourself daily. Usually more than once a day.
The precise type/make of medication (as well as the dosage) you take will depend on a number of factors – some of which are unique to you (such as your LH and FSH levels), and some of which are just down to cost and doctor preference. Some people will be put on different medication for round 2 if round 1 was unsuccessful and caused any particular problems (e.g. iffy side effects, bad-quality eggs, or an unusually long time for follicles to increase in size).
What happens after I begin the injections?
You’ll spend a lot of time with a cold, dildo-shaped wand up your whoojamaflip and a syringe that drains blood from your arm. Fun times.
Basically: don’t plan any holidays during this time. And ideally don’t have a job, either, because it really gets in the way of all your medical appointments. (I’m freelance and work from home, and I have no bloomin’ clue how people in regular jobs manage.)
The scans: why and when
As a result of Step 1, you’ll no doubt already be on first-name terms with the dildo-shaped wand (mine was called Stan), but prepare to get seriously familiar with it over the next couple of weeks. We’re talking frequent transvaginal ultrasound examinations (scans) here: twice a week if you’re lucky, daily if you’re not.
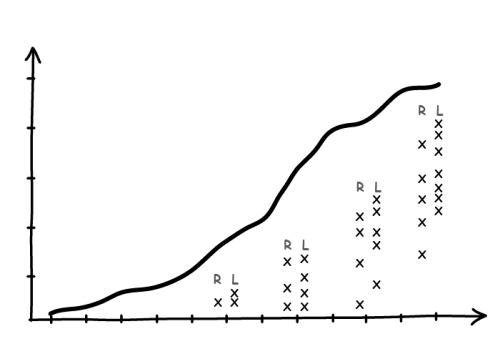
Stan (also known as a “dildocam”) is there to check on the follicles growing in your ovaries – both how many and what size. (Your eggs can’t be seen on the scan because they’re microscopic in size, so the size of the follicle is used as a proxy.) The results are plotted on a graph on a piece of paper.
While downregulation/taking over your menstrual cycle allows all follicles to grow at roughly the same speed, your ovaries still like to prove that they have a degree of freedom in the process – and as a result, there’ll be some variation in the sizes of your follicles. The doctors’ aim is to end up with at least ten follicles that are approximately 15–24mm in diameter – i.e. follicles containing eggs that are deemed ready for ovulation.
Most doctors actually prefer to wait until at least a few follicles have reached at least 18mm: at 15mm, the eggs inside still might not be ready for ovulation. On the other hand, the follicles can’t be left to grow for too long: go past 24mm and there’s a risk that the eggs will be too “ripe” and therefore can’t be used.
It has to be timed beautifully, basically. And it’s why you might need to go in for multiple sessions with Stan over the course of the ovarian stimulation process.
The blood tests: why and when
The blood tests check your oestradiol level. Oestradiol levels rise during a “normal” non-IVF cycle – and they’ll rise by a greater amount in an IVF cycle because you’re growing more follicles (and the cells inside each follicle produce oestradiol).
But having a sky-high amount of the stuff means you’re at risk of ovarian hyperstimulation syndrome (OHSS). Having lots and lots of large follicles is usually an indicator that your oestradiol level will be elevated, because the cells in each large (>15mm) follicle will produce around 200–500 pg/ml of oestradiol.
- The dream scenario: approximately 15–20 follicles (18–24mm), and an oestradiol level between 2,000 and 4,000 pg/ml.
- Getting worrisome: more than 20 follicles (18–24mm), and an oestradiol level between 4,000 and 6,000 pg/ml.
- Eeek: more than 30 follicles (18–24mm), and an oestradiol level above 6,000 pg/ml.
Read more about oestradiol levels here.
Your medication will be adjusted according to how well your follicles are growing and whether you seem to be at risk of developing OHSS. (Some people are even told to “coast” for a few days – which means “lay off the drugs for a while to let your oestradiol level settle down and make sure you’re not growing any more follicles”.) Read the page on OHSS for much more information about all this.
What happens if you have a fudgeton of eggs and your oestradiol level refuses to calm down? There’s a chance you’ll have to stop this IVF cycle and start again from scratch. Sorry: no easy way to say that.
How do the doctors make sure I don’t ovulate by accident?
There are probably many things worse in life than spontaneous ovulation, but… who are we kidding? That would be the ultimate kick in the teeth, right? You go through all this hassle and pain to create an impressive basketful of eggs, and then out of nowhere they decide to mature and pop out of their follicles when no one’s around to catch them.
Thankfully, there’s a solution for this. Less thankfully, it involves yet more injections…
- If you’re on the long protocol (i.e. downregulation), you’ll be instructed to continue taking your ovulation-preventing “gonadotrophin-releasing hormone (GnRH) agonists” – Lupron, Suprecur, Synarel, etc. – while stimulating your ovaries.
- If you’re on the short protocol, you’ll start taking similar drugs to the GnRH agonists – except these ones are called “GnRH antagonists”. Names for these drugs include Cetrotide and Antagon, and you’ll start taking them once some of the follicles have reached a certain size – around 14mm. Unlike the agonists, these injections get to work right away at preventing ovulation. That’s why you didn’t need to start taking these drugs for a couple of weeks before the ovary stimulation phase (unlike those on the long protocol).
The GnRH agonists and antagonists prevent spontaneous ovulation in slightly different ways – ways that you don’t need to worry about right now. Just know that they’ll rein in your eager eggs until everyone’s ready for them.
IVF #3: ovulation
- The goal: get your eggs ready for retrieval!
- Approximate time taken: 1 injection
- Approximate number of appointments needed: 0
- Potential side effects: headache, irritability, sore breasts, mild fluid retention and weight gain (but also be aware of symptoms of OHSS)
A big moment: at this point, you have plenty of follicles that are the right size, which means you also have plenty of eggs that are almost ready for retrieval! What’s more, the lining of your uterus has grown to be nice and thick, to form a comfortable cushion for the embryo that will be placed there shortly.
All you need to do now is get those darn eggs out of you.
An imaginary discussion with your ovaries shall now commence…
You: Hello, Ovaries. It’s ovulation time! You excited? Yeahhhhh, course you are!
Ovaries: Hang on just one sweet second… you’ve been doing everything in your power to stop me from ovulating (I wasn’t allowed to release even one teeny egg), and now you’re suddenly acting like ovulation is the best thing since crossword toilet paper? What happens if I don’t want to ovulate?
You: It’s called “doing a one-eighty”, and you just have to deal with it. (But thank you ever so much for your service thus far. Seriously: great job.)
How do I trigger ovulation?
You’ll be given a time slot to go into the clinic for egg retrieval, and you’ll be asked to give yourself a special “trigger” injection a precise number of hours (it’s usually 36 hours) before that slot.
You know how medication pamphlets often provide warnings like “Don’t operate heavy machinery while using this medication”, or “Don’t take with alcohol”? And you just think “Screw that: I have a forklift to drive and a wedding to attend, so I’m damn well taking this Benadryl anyway”? We’ve all been there. But when it comes to your trigger shot, pay attention to the instructions provided by your doctors. You MUST inject yourself at precisely the right time – and you MUST heed their warnings about all the stuff you need to do beforehand. The reason will become clear in a sec.
Where was I? Oh yes: the trigger injection. This completes the final process of maturing the egg (known as “meiosis”) and causing ovulation. There are two main types of trigger injection, and the one you have will depend on a few different factors:
- The hCG trigger injection is used by people who’ve been on both the short and the long protocol. hCG stands for “human chorionic gonadotrophin”, and it’s the same hormone that’s released at the start of pregnancy. So what’s it doing at this stage of the IVF process, you might ask, before anything’s been fertilised?
Well… hCG is very similar to LH – which is what stimulates ovulation in “normal”, non-IVF cycles. hCG can have a similar stimulatory effect in people undergoing IVF – especially for those whose natural LH level has been suppressed through downregulation. - A GnRH agonist (such as Lupron) is often used for people who’ve been on the short protocol. It causes the release of a natural LH surge – which is what happens with a “normal” cycle to induce ovulation. If you have so many follicles that you’re verging on too many, a GnRH agonist will reduce the risk of OHSS compared to hCG.
Wait… back up a second. The hormone that helped to prevent ovulation in long-protocol patients is now being used to stimulate ovulation in short-protocol patients? WTF? Yes indeedy. You see, drugs like Lupron cause a MAHASSIVE LH (and FSH) surge when you start taking them, but that doesn’t matter during downregulation because the injections are given after an egg has been released by the ovaries. (If given beforehand, the drug can induce ovulation – like it does when used as a trigger.) Then after a week or so of taking the Lupron, the body gets overwhelmed by all the LH and becomes densensitised to it… which has the effect of stopping FSH, LH and oestradiol production.
When you take a single GnRH agonist dose after stimulation, on the other hand, you’ll get the LH surge right when you need it.
The GnRH agonist seems safer for everyone, so why not just use it on us all? Well… not all patients respond to it – especially those who’ve undergone downregulation or have an insufficient natural LH level. Another reason is that the surge caused by a GnRH agonist isn’t as long as you’d get with a natural menstrual cycle or hCG. While that's great if you’re at risk of OHSS (the longer the surge, the more oestradiol will be released – and there’s a link between oestradiol levels and OHSS), it also means the lining of your uterus (which needs oestradiol to develop) might not become thick enough for embryo implantation. As a result, you’d probably have to do a frozen embryo transfer (FET)… and you might not want to wait.
Some people will have a dual trigger – part hCG, part GnRH agonist – which reduces the likelihood of a shitty response while keeping the risk of OHSS low.
What happens after I’ve had the trigger injection?
The countdown begins until egg retrieval time! As mentioned above, you’ll have been given a specific time to arrive at the clinic/hospital, which will be a specific number of hours (usually around 36 hours) after the trigger injection.
Here’s why: ovulation takes place approximately 36 hours after the trigger injection gets into your system (which takes a bit of time in itself). The doctors need to collect your eggs just before ovulation takes place, but just after the eggs are fully developed and ready. It’s a teeny tiny window of time, and if you miss it, you’re screwed.
You mustmustmust do what the doctors say when it comes to the time you take your trigger and the time you arrive at the hospital/clinic: they’re being strict for a reason.
Another rule? You’ll be told to fast from midnight the night before your egg retrieval – including chewing gum and sweets – and to stop drinking four hours before the procedure. This is to protect your own health. Well, I say “health”, but what I mean is “life”: you’ll be heavily sedated or anaesthetised while the eggs are collected, and food or drink in your system can cause something called “aspiration”. I won’t explain it all here, but Google it if you want the deets.
IVF #4: egg (and sperm) retrieval
- The goal: get those eggs out of you!
- Approximate time taken: 20 minutes for the actual procedure, plus an hour or so for “recovery” before you’re allowed home
- Approximate number of appointments needed: 1
- Potential side effects: general bleurghness from sedation, soreness “down there”, cramping, insaaane constipation, ovarian torsion, OHSS
The big day! You’ll need to book the morning off work, but plenty of women choose to take at least the full day off. If you’re going to come down with OHSS (which usually kicks in a few days after egg retrieval), you’ll need a good week at home – more if you have the “serious” kind.
You’ll arrive at the clinic, fill in a bunch of forms, swear on your life that you haven’t eaten since midnight or had anything to drink since the crack of dawn, and be instructed to change into a hospital gown.
Then you’ll be wheeled into theatre and be put under heavy sedation or general anaesthetic (depending on the clinic/hospital) while the doctor makes lame jokes in a sweet attempt to calm your nerves. Then… blankness. You’re out for the count while they get at your eggs.
Here’s what happens:
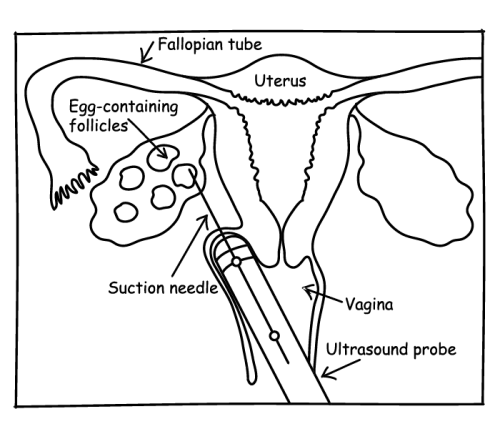
- They’ll pass a needle through the top of the vagina to get to the ovary and follicles. Ultrasound guidance helps them find the exact spot.
- Next they’ll “puncture” (my word, not theirs) the follicles so that the eggs detach from the follicle walls and can be sucked out of the ovary.
- The eggs will be taken to the IVF lab, ready for fertilisation.
- You’ll wake up feeling a bit crampy, a bit moody and possibly a bit hungry.
For LOTS more detail about egg collection (including the experiences of people who've been through it), read “Egg collection for IVF: all your questions answered“.
Meanwhile…
I haven’t mentioned what your partner’s up to while your precious insides are being poked and prodded by a massive needle. He’s having a marvellous time: watching porn, reading fetish websites, fantasising about Scarlett Johansson and jizzing away happily in his own private wank-off room.
(That's not quite true – and many men find the sperm collection process to be quite an ordeal. If your partner is worried or has any questions, send him a link to “Sperm collection: what you need to know (an article for the men)“.)
You’ll then both be told how many eggs were retrieved and how good the sperm sample looks. Then it’s time to go home and REST!
A few hours after egg retrieval (and depending on the quality of the sperm sample), your eggs will be mixed with the sperm.
Worried you'll never remember all this information? Click here to download a quick printable summary of the entire process – plus a jam-packed IVF glossary. (Opens in a new window.)
IVF #5: fertilisation & embryo development
The day after the eggs and sperm have been mixed, they’ll be checked to see how many have fertilised (approximately 70% of eggs will normally fertilise). At this stage they’re called embryos, and they’ll be monitored constantly to see how they develop.
The embryos will spend up to six days inside their own personal incubators, and you’ll be phoned each day with an update on both their progress and when the most suitable day for transfer might be (if you’re doing a fresh embryo transfer rather than a frozen one). Some embryos will be better quality than others, and it’ll be one of the good ones that they transfer into your uterus.
IVF #6: embryo transfer
If you’re doing a fresh embryo transfer, you’ll probably start taking progesterone (and maybe oestradiol) the day after your egg retrieval, in order to keep the lining of your uterus thick. Then a few days later, one embryo (perhaps two) will be transferred back into your uterus. Any remaining embryos can be frozen for later use.
If you’re doing a frozen embryo transfer, you’ll have had a break since egg retrieval. First, you’ll take medication to induce a period (so that your cycle can be controlled more precisely and an embryo transferred at exactly the right time). Once your period arrives, you’ll start taking oestradiol to thicken your uterus lining, and another drug (called a GnRH antagonist) to make sure you don’t ovulate. You’ll also be prescribed progesterone (for the same reason as the oestradiol) – but that won’t start until closer to “embryo transfer” day.
Once the lining of your uterus is the right thickness, one of your frozen embryos will be thawed and transferred into your uterus.
- Find about more about fresh embryo transfer vs frozen embryo transfer.
- If you want to know about my own experience of the embryo transfer itself, read point #7 here.
And there you have it: the main part of the IVF process explained!
Want to help support The Duff?
The Duff is a pure passion project, and it will always be free – so your support goes a long way.
If you'd like to help me keep researching and writing about IVF and fertility in my spare time, you could consider making a one-off small donation: whether you give £2 or £20, I'll be hugely grateful.
(After you click, you'll be taken to a new tab where you'll be asked to donate however much you like to The Duff/Team Incredible. “Team Incredible” is the official company name. Long story.)