OVARIAN HYPERSTIMULATION SYNDROME (OHSS) IS A NASTY, NASTY BEAST OF A MEDICAL CONDITION – one that could land you in hospital and significantly delay any planned fresh embryo transfers.
(And while I don’t want to freak you out for the hell of it, OHSS can kill you. So, you know, take it seriously.)
Here's what you need to know:
What exactly is OHSS?
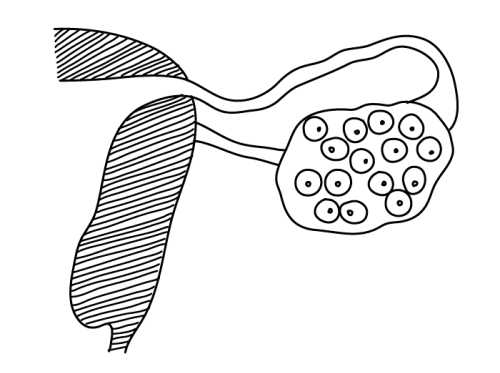
It’s a complication of fertility treatment – particularly IVF – that causes your ovaries to swell, fluid to build up around your tummy, and a nice bunch of accompanying symptoms.
What causes OHSS?
Too many follicles, usually. When your ovaries are stimulated to produce follicles during IVF, there’s a risk you’ll produce “too many” follicles. If you’re young, have PCOS or a low BMI, or a few other risk factors mentioned shortly, you’re more likely to overstimulate and produce all those follicles.
How is OHSS caused by “too many follicles”?
OK so this is bloomin’ complicated and it appears that medical specialists still aren’t entirely clear on what’s going on, but here’s the general gist:
At the “ovulation” stage of every menstrual cycle, there’s a hormone surge that causes the egg to break free from its follicle so that it can travel into the fallopian tube, ready to be fertilised. In a natural cycle, the hormone is LH; in an IVF-assisted cycle, the hormone is often hCG – which acts in very similar ways to LH. (If you want more detail about all this, read my mega-post about the entire IVF process.)
The hormone surge also acts as a signal to the ovaries to produce new and temporary capillaries. In a natural cycle, these capillaries invade the cells of your leftover ovarian follicle (the one that used to contain the egg), in order to deliver cholesterol to those cells. Why? Because then the cells can produce progesterone (which is made from cholesterol), which will help to sustain the lining of the uterus in case there’s a pregnancy.
These capillaries need to be made super quickly, and as a result, they wouldn’t even pass the requirements of a corrupt building official in Turkmenistan: they’re pretty darn leaky. The fluid portion of the blood leaks through the capillary wall, but it’s not really a biggie when you only have one dominant follicle (as you would with a natural cycle): there won’t be too many capillaries, and therefore there won’t be too much leakage. What’s more, the important stuff – the cellular portion of the blood – stays in the capillaries and does what it needs to do.
See where I’m going with this?
When you have lots of follicles (caused by fertility treatment), you have lots of capillaries – and all the fluid from the blood leaks through the capillary walls. This time there’s LOADS more fluid, and it all kind of swirls around in your abdomen with nowhere to go. The ensuing symptoms are a treat.
What are the symptoms of OHSS?
There are three levels of seriousness:
Mild (up to 33% of women who do IVF):
- You have a mild build-up of fluid in your abdomen, which causes bloating/swelling, abdominal discomfort, nausea, cramps and heartburn/indigestion.
- Your ovaries are enlarged/”stretched” (usually by less than 8cm) in response to overstimulation, which causes more abdominal discomfort.
- You experience mild weight gain caused by the fluid build-up (but less than 1 kg per day).
Moderate:
- There’s more of a build-up of fluid in your abdomen (called “ascites” if the fluid exceeds a certain amount) compared to mild OHSS, and this produces even more pronounced bloating/swelling, abdominal discomfort, heartburn/indigestion, cramps and nausea/vomiting.
- Your stomach may be distended.
- Your ovaries are enlarged/”stretched” (8–12cm) in response to overstimulation, which causes more abdominal discomfort.
- You experience weight gain caused by the fluid build-up (but less than 1 kg per day).
Severe to critical: (about 1% of women who do IVF):
- You have so much fluid (“ascites”) that it continues travelling up your body and ends up interfering with your diaphragm’s ability to move – making breathing difficult.
- The pressure from all the fluid makes your stomach feel incredibly bloated, “full” and painful.
- Your stomach will probably be distended.
- Your blood volume decreases as a result of all the fluid leakage, which in turn might cause the kidneys to slow down their production of urine. Decreased urine output (defined as less than 30 ml of urine per hour) is considered a pretty serious symptom of OHSS.
- Your blood viscosity increases as a result of the fluid portion leaking through the capillaries, leaving the cellular portion highly concentrated. This can put you at risk of blood clots in the veins and lungs (thrombosis).
- Your ovaries stretch like crazy (more than 12cm) in response to the overstimulation, which brings about the same abdominal discomfort as moderate OHSS – but worse.
- Very rarely, there might also be ovarian torsion – where the overstimulated ovary twists around itself, cutting off its blood supply. I felt ill just writing that sentence.
- You get all the same crampy, bloating, heartburny symptoms as mild and moderate OHSS – but worse.
- You feel weak and faint because of the reduction in circulating blood volume.
- You experience significant weight gain caused by the fluid build-up (approximately 1 kg per day or more).
When will the symptoms of OHSS appear?
There are two time periods during which you can start to experience symptoms:
- With “early onset OHSS”, symptoms can appear within 24 hours of the hCG trigger, but it often takes anywhere up to nine days before they become really apparent. (Basically, don’t do what I did – which was to wake up the day after 41 eggs were retrieved from my ovaries and smugly state, “If I have OHSS, it’s SO no big deal! All those women moaning on various message boards are such wusses.” Two days later I was in hospital with a catheter in my urethra, a drip in my arm, and a tummy the circumference of an out-of-shape sumo wrestler.)
- With “late onset OHSS”, symptoms appear after a successful fresh embryo transfer – which usually takes place up to ten days after egg retrieval (once your eggs have been mixed with sperm. It’s a bit of a double-edged sword, this one: you’re pregnant, but you also immediately look pregnant (and feel horrific) because you now have OHSS. The reason you get late onset OHSS? Because after the hCG has justjustjust surged through your system thanks to the trigger injection, you get another hefty dose of the stuff – this time produced naturally by your body – when you become pregnant. If you had two embryos successfully transferred, you get to feel doubly elated and doubly shit.
If you get early onset OHSS, you’re very likely to also get late onset OHSS – and late onset OHSS tends to be more severe and more longlasting (up to 12 weeks, at which point the body’s natural hCG levels begin to die down). It’s for this reason that you might be advised to freeze all your embryos and wait for your body to calm down before the embryo transfer.
(If your doctors are aware from the start of treatment that you have a high risk of developing OHSS, you may be advised to do a frozen embryo transfer before they’ve even done the egg retrieval. That’s because you could, in theory, do the egg retrieval, feel absolutely fine, then proceed with a fresh embryo transfer without realising you were on the verge of some mothereffing OHSS symptoms.)
What type of people are likely to get OHSS?
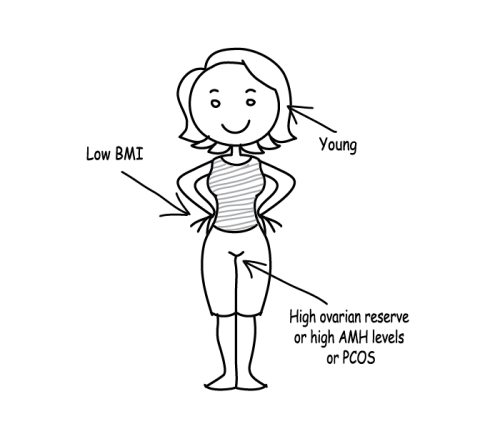
Consider yourself more at risk if any of the following apply to you:
You’re young (under the age of 35)
This is possibly because you have a higher number of follicles remaining in your ovaries plus a greater density of hCG receptors.
You have a low BMI
No one really knows why this is a factor.
You have a high ovarian reserve
“Ovarian reserve” has two separate components. The first is the actual number of follicles that you have in your ovaries. (Age has a big influence on your follicle count, but so does genetics, tobacco usage, and previous ovarian surgery.)
The second is the actual health of the follicles and the eggs within them. Again, age is a biggie here: the younger you are, the more likely it is that you’ll have high-quality eggs.
A high ovarian reserve increases your chances of successful fertility treatment, but it also increases the likelihood that you’ll get OHSS.
Read more about age, egg quality and egg quantity here.
You have polycystic ovary syndrome (PCOS)
You already have a larger number of follicles in your ovaries compared to the average person (although these follicles tend not to mature and ovulate properly), and you have a tendency to overrespond to certain hormones. These two things combined mean you have a greater chance of growing a large number of follicles.
You had a high level of anti-Müllerian hormone (AMH) before starting IVF treatment
A high AMH level (determined with a blood test) is considered to be one of the best predictors of an OTT response to stimulation. High AMH is normally connected with PCOS and ovarian reserve. Read more about AMH levels here.
You’ve had OHSS before…
… Or you overresponded to another type of fertility treatment (e.g. Ovulation Induction) – even if you didn’t actually end up with OHSS itself.
Remember, though: these are just risk factors, and anyone can succumb to the delights of OHSS.
Is OHSS preventable?
Ish. Doctors can usually detect if you’re likely to get it by looking at the following:
- Your risk factors before treatment (see above).
- Your oestradiol levels (measured with frequent blood tests) while undergoing treatment. Oestradiol is a type of oestrogen, and having a sky-high amount of the stuff means you’re at risk of OHSS.
- The number of follicles you’re producing while undergoing treatment. Having lots and lots of large follicles is usually an indicator that your oestradiol levels will be elevated because each large (>15mm) follicle will produce around 200–500 pg/ml of oestradiol. In an ideal world, IVF treatment will result in approximately 15–20 follicles (18–24mm), and oestradiol levels between 2,000 and 4,000 pg/ml. Things get worrisome when you have more than 20 follicles (18–24mm), and oestradiol levels between 4,000 and 6,000 pg/ml. Doctors do not like to see more than 30 follicles (18–24mm), and oestradiol levels above 6,000 pg/ml.
It's also possible to have high oestradiol levels without a large number of follicles – and that's still an indication that you might get OHSS (although from what I can tell, doctors aren't completely sure why).
Once doctors have looked at all these things in conjunction with each other, they’ll often be able to nip OHSS in the bud before it happens – or at least ensure you’re not going to get a severe case of it.
They have a few ways of doing this:
- Going short. If you clearly have a high risk of developing OHSS before beginning IVF treatment, you’ll probably be put on the “short IVF protocol” (rather than the “long IVF protocol”), because it involves drugs that reduce the risk of OHSS. This includes the drug used to trigger ovulation: instead of hCG, something called a “GnRH agonist” is used instead. (Read more about it in this post on the IVF process.)
- Trigger happy(ish). If you were considered “low risk” (and therefore on the long protocol) but you start to show signs of developing OHSS anyway, your doctor may adjust down the amount of follicle-stimulating medication you’re taking. They may also decide to decrease how much hCG you take to trigger ovulation. (Some doctors believe that a reduction in hCG leads to reduced egg quality, but others think it does no harm whatsoever.) Another option is to give you the same trigger injection that those on short protocols are given – but many doctors agree that this is usually ineffective among patients who’ve been on the long protocol up to this point.
- Polycystic, polyshmistic. The use of “insulin-sensitising agents” such as metformin has been shown to help prevent OHSS in women with PCOS.
- Aiming for a soft landing. If you rapidly develop high oestradiol levels (>4,000 pg/ml) combined with lots of follicles (more than 20), your doctor may tell you to stop taking your follicle-stimulating medication and wait a few days before taking the trigger injection. This is known as “coasting”.
- The big freeze. If you’re growing a large number of follicles but the doctors are confident they can stave off severe OHSS through some of the methods above, they might continue with the egg retrieval but tell you to freeze ALL embryos (rather than do a fresh embryo transfer a few days later). This is to prevent the “double surge of hCG” mentioned earlier.
- Abandon mission (sadface). If your body goes apeshit with tons of follicles, super-high oestradiol levels, and you’re already feeling bloated and horrid, there’s a chance you’ll have to abandon the cycle and start again with a new IVF cycle. This is an ultimate last resort, though.
One or more of these methods should ensure you only end up with mild OHSS at the very worst. But, well, some people aren’t so lucky. Take me: I was considered “high risk” and – as predicted – my oestradiol levels went through the roof and I grew a ton of follicles. My doctors were prepared: I'd been told from the start that I’d be freezing all embryos after egg retrieval, due to the fact that embryo transfer would worsen any (hopefully mild) OHSS symptoms that might appear. And when my oestradiol levels climbed to what they considered a dangerous level, I “coasted” for a few days before having the GnRH agonist trigger injection.
And yet I still ended up in hospital with moderate/severe OHSS. Leaky capillary fluid collected all over my abdomen and higher up, making it hard to breathe. I gained 5 kg in five days. Eating was agony. I was up all night with stomach cramps. My waist size ballooned. My ovaries were ginormous (as seen on a scan). And oh goodness the tightness… no one had really told me about the tightness: it felt like my organs were going to burst out of my skin at any moment. It wasn’t the best experience ever.
(Gosh: that was the most typically British sentence ever. For any non-Brits reading this, what I mean is, “It was the goddamn worst.”)
This isn’t to scare you or make you feel like any of the preventative measures above will do bugger all – just that you can never get rid of the risk completely.

I have OHSS. How do I get rid of it?
Unfortunately, despite taking all manner of precautions, you may still end up with OHSS. When it comes to how to treat it… there's both good and bad news. As is tradition, let's start with the bad.
The bad news is that the answer is “nothing”. There’s absolutely nothing you can do to “get rid of” or “cure” OHSS. The good news is that the condition is “self-limited”: it will run its course, which usually takes around two weeks. After the trigger injection, you’ll have no reason to inject any more of the stuff, so you’ll have no more hormone surges and the OHSS will clear up.
That’s not to say you won’t need monitoring and/or treatment, of course (especially for some of the worse symptoms, which could lead to severe medical problems of their own) – just that it’ll definitely go away at some point soon.
If you’re pregnant and you have late onset OHSS, your symptoms too will be self-limited; it’s just that it’ll take a lot longer because it takes longer for the hCG to leave your system.
What kind of monitoring/treatment might I need for OHSS?
That depends on how badly you’re suffering. Bizarrely, it also seems to depend on where in the world you live: doctors in the USA and UK seem to have very different opinions on how you should self-treat mild OHSS.
For mild/moderate OHSS…
Tell your clinic about your symptoms, as they may want to scan you in order to see just how large your ovaries are and how much fluid has collected in your abdomen. If they agree that your symptoms are mild/moderate, you can probably self-treat at home (although you may still be monitored as an outpatient – especially if you plan on having a fresh embryo transfer).
Self-treatment advice given by UK doctors (NHS and private) is usually as follows:
- Make sure you’re drinking enough water: your blood has lost a lot of fluid and is much more concentrated as a result, which makes your kidneys slow down (and can also cause dehydration). Water will help to rehydrate you and bring some fluid back into the blood. You ideally need to be drinking enough that you’re peeing out pale yellow urine every two hours.
- Eat plenty of protein, which will help with the production of albumin – a component of blood that helps to keep the fluid part of the blood from leaking out of the capillaries. Some people also believe that protein makes the capillaries more substantial and inherently less leaky.
- Take paracetamol or codeine to manage the pain (although if you think your constipation was bad before the codeine…). Don’t take any NSAIDs (nonsteroidal anti-inflammatory drugs) like ibuprofen or aspirin, because they can have a bad effect on your already-delicate kidneys.
- Avoid all strenuous activity to make sure you don’t accidentally get your now-MASSIVE ovaries in a twist (quite literally). Many online sources specifically state that you should avoid sex, but they really needn’t bother: OHSS is more mood-dampening than an early-morning call from your mother-in-law about her varicose veins.
- On the other hand, don’t just sit in bed for two weeks doing nothing but eat your weight in eggs and tuna: move around and do gentle walking to help avoid blood clots.
- If you hadn’t already been prescribed anti-coagulation/blood-thinning drugs (known as low-molecular-weight heparin, or LMWH) in anticipation of OHSS, you might be told to start taking them now. Brand names include Fragmin, Clexane and Lovenox, and they’re taken as injections.
- Weigh yourself at the same time every day to monitor for rapid weight gain (more than 1 kg per day).
- Monitor how often you’re urinating, and what colour your urine is.
- Get yourself to a doctor (or hospital) if your weight is increasing significantly and you’re not urinating anywhere near as often as normal.
If you find yourself on any American message boards or blogs, you’ll likely find that the advice given to patients there differs in three main ways. Firstly, they’re generally told NOT to drink pure water, but to have fluids containing electrolytes instead. (Gatorade gets mentioned a lot, and coconut water gets the nod from people who are freaked out by the sugar content and overall artificial-ingredientness of Gatorade.) That’s because they provide sodium and potassium – which are being lost in the fluid from your blood leaking out of your capillaries.
Secondly, American doctors encourage you to go crazy in general on your salt (and therefore sodium) intake. Apparently, this isn't just to address the electrolyte imbalance, but also due to reasons relating to osmosis: salt encourages the fluid out of your abdomen and into your bloodstream.
Thirdly, many American doctors recommend that you take aspirin daily to help avoid blood clots. Aspirin is an NSAID – which British doctors specifically instruct you to avoid. So… yeah.
I asked my NHS doctor about the American advice regarding fluids and salt (I hadn’t heard about the aspirin thing at that point), and she looked both alarmed and angry. Heaven knows how she hadn’t heard about this conflicting advice, but she didn’t seem to think that a buttload of salt and sugary drinks would help in any way whatsoever.
My opinion? OHSS will clear up when it will clear up. You can eat a Chinese takeaway with a side of salt ‘n’ vinegar crisps every night or plain chicken with rice, and it will still clear up in its own time. You can drink water or Gatorade/Lucozade, and it will still clear up in its own time. Judging by the “It worked for me!” comments from people on both sides of the Atlantic, it’s all placebo. (Although please remember this is JUST my very cynical opinion.)
When it comes to aspirin, though, check that one with your doctor.
For moderate/severe OHSS…
If you’re doubled up in pain to the extent that you’re thinking, “This has GOT to be worse than childbirth,” if you’re struggling to drink water because it makes you feel too sick, if you’re putting on more than 1 kg per day, and/or if you’re struggling to breathe due to all the fluid flowing up through your body, you may well be admitted to hospital in order to be monitored more closely.
Your condition is still “self-limited”, but doctors at the hospital can do a few things to hasten your recovery, make you feel more comfortable, and ensure some of the symptoms don’t develop into bigger problems of their own:
- If you can’t drink fluids due to nausea, you may be given an intravenous drip (IV) instead.
- Some patients are catheterised so that doctors can monitor fluid in vs fluid out (which helps them determine the seriousness of your dehydration and general condition).
- If you’re not urinating as much as you should be, and if the IV doesn’t improve matters, you’ll also be given an albumin solution to bulk up the blood (for the same purposes as eating protein – see above).
- More hardcore pain relief medication will be available, such as pethidine.
- You’ll be given a pair of those super-sexy DVT socks to reduce the risk of blood clots.
- … And you might also be prescribed anti-coagulation/blood-thinning drugs (known as low-molecular-weight heparin, or LMWH) for the same reason – if you’re not taking them already. There are a few different brand names, including Fragmin, Clexane and Lovenox, and they’re taken as injections.
- Your waist will be measured daily to check that the fluid in your abdomen is decreasing.
- Very occasionally, the fluid in your abdomen will be drained off to make you feel more comfortable. It’s called “paracentesis”, and it involves inserting a thin needle/tube into your tummy under a local anaesthetic. It doesn’t “cure” anything or prevent further build-up, but it’ll make you feel better for a while.
Can I still do the embryo transfer if I have OHSS?
Most doctors advise against it – and I would too, if you have anything worse than very mild OHSS. Give your body a chance to recover, and then do a frozen embryo transfer a couple of months later. (Success rates for frozen embryo transfers are on par with fresh ones these days.)
OHSS: all you need to know!
The good, the bad and the ugly.
“The good?” you say. “The GOOD???” Well, OK, this is a bit of a self-indulgent and thoroughly non-universal “good” that I managed to eke out of the whole palaver: my husband ADORES hospital food, so it made me all kinds of happy to see him polish off my lukewarm chicken tikka masala and sponge pudding after he’d spent the past few days worrying like hell about me.

